How to Read a Mri of Ankle Posterior
Links To Diagnostic Imaging Pages [edit | edit source]
Diagnostic Imaging for the Physical Therapist
Diagnostic Imaging of the Hip for the Physical Therapist
Diagnostic Imaging of the Human knee for the Physical Therapist
Introduction: [edit | edit source]
In improver to a thorough history and clinical exam, imaging may be helpful in diagnosing and creating a plan of intendance in a patient with a human foot or ankle injury. Imaging of the pes and talocrural joint can be beneficial to rule in or rule out pathology after trauma to the human foot or ankle or when an injury is not progressing with conservative management. For bony pathology, in that location are iii standard views for a radiograph. The AP view is projected through the body of the talus and distal tibia. The lateral view demonstrates the joint of the distal tibia and talus, too as a lateral view of the calcaneus and tarsal basic. The mortise view displays the talus and the distal tibia without overlay from the fibula. If instability is suspected a stress image can exist taken to determine ligamentous laxity. If soft tissue damage or tissue inflammation is suspected an MRI or diagnostic ultrasound may exist indicated. [1]
Hallux Valgus: [edit | edit source]
Hallux Valgus is a deformity where the neat toe deviates laterally and the 1st metatarsal deviates medially to create a valgus angle at the 1st MTP joint. Considering this is a bony deformity a radiograph is the gilded standard for determining Hallux Valgus. [2]
Reading a radiograph for Hallux Valgus [edit | edit source]

Radiograph of Hallux Valgus
Reprinted from [ii]
- Preferred radiograph view is a dorsoplantar view in weight bearing.
- The valgus angle is measured from the 1st metatarsal to the nifty toe. An angle >xv degrees is considered a hallux valgus deformity. [iii]
Lateral Ankle Sprain: [edit | edit source]
The lateral ankle ligaments are involved in 95% of talocrural joint sprains.[ane] In lateral ankle sprains, 66% are isolated tears of the anterior talofibular ligament (ATFL), 20% accept associated calcaneofibular ligament (CFL) sprains and the posterior talofibular ligament (PTFL) is rarely involved[3]. Imaging for a lateral ankle sprain may be indicated through machinery of injury, location of pain and positive special tests (anterior drawer and talar tilt test). A study comparison the diagnostic accuracy of MRI, ultrasound, and stress radiograph to the "gold standard", arthroscopic surgery, plant accuracies of 97%, 91% and 67%, respectively in determining tears of the ATFL. The written report also compared the ability to determine location of the tears and plant that MRIs could accurately tell the location of the tear in 93% of cases and that ultrasound could tell the location in 63% of the cases. [4]
Reading an MRI for lateral talocrural joint sprains [four] [edit | edit source]

T2 Weighted Axial paradigm of ATFL tear
Reprinted from http://world wide web.radsource.usa/dispensary/0308
- Typically a T2 weighted image from an axial view is used to observe tears in the ATFL.
- Ligamentous injury is indicated if there is aperture, a wavy or curved contour or increased betoken intensity inside the ligament.
Reading an ultrasound for lateral ankle sprains [4] [edit | edit source]

Ultrasound epitome of ATFL tear
Reprinted from http://web log.naver.com/PostView.nhn?blogId=narssen0&logNo=120065795408&redirect=Dlog&widgetTypeCall=true
- Imaging is performed with the talocrural joint in slight plantar flexion and inversion to put a stretch on the ATFL
- Ligamentous injury is indicated if there is aperture of the ligament or the ligament is hypoechoic.
Syndesmotic (High) Ankle Sprain [edit | edit source]
A syndesmotic ankle sprain occurs when at that place is an injury to the anterior inferior and posterior inferior tibiofibular ligament and/or the interosseus ligament. Syndesmotic talocrural joint sprains are more mutual in contact sports and typically occur with external rotation of the tibia on a dorsiflexed ankle on a planted pes. [3] Clinical indications of a syndesmotic ankle sprain may exist the mechanism of injury, pain at the distal tibiofibular joint and positive special tests (dorsiflexion external rotation test, squeeze examination and cotton test). If a syndesmotic talocrural joint sprain is suspected the initial imaging selection may exist three view radiographs taken in unmarried leg continuing. Radiographs can be beneficial in determining an osseus avulsion, which is present in 50% of syndesmotic ankle sprains, and to determine syndesmotic widening. AP and mortise view radiographs have been shown to accept 100% specificity, but poor sensitivity. If a syndesmotic sprain is non indicated on a radiograph, but there are however questions regarding the diagnosis an MRI may be indicated. [5]
Reading a radiograph for syndesmotic ankle sprains [5] [edit | edit source]

Radiograph of syndesmosis
Reprinted from http://www.aafp.org/afp/2001/0101/p93.html
- iii views taken in single leg weight bearing.
- Await for osseus avulsions in the anterior or posterior aspects of the tibia
- Await for gapping or "articulate space" in the posterior attribute of the syndesmosis. >5 mm measured on an AP or mortise view is considered abnormal.
Reading and MRI for syndesmotic talocrural joint sprains [5] [edit | edit source]

T2 axial view of anterior tibiofibular ligament disruption
Reprinted from http://www.radsource.us/clinic/1007
- An centric view of T1 and T2 weighted MRIs can be indicated to determine syndesmotic ankle sprains.
- Positive MRI findings for syndesmotic ankle sprains on a manifestly T1 or T2 weighted image are aberrant class, irregular contour or increased signal intensity.
- A positive finding on a T1 weighted image with contrast is marked signal intensity.
- Boosted positive findings with be discontinuity or not beingness able to visualize the ligament.
Foot and Ankle Fractures [edit | edit source]
If a foot or talocrural joint fracture is suspected it is recommended to employ the Ottawa Ankle Rules to screen whether a radiograph is needed. The Ottawa Talocrural joint Rules point that a radiograph is indicated if any of the following are positive: tenderness forth the posterior medial or lateral malleoli, base of the 5th metatarsal, navicular or if the patient is unable to carry weight for 4 steps following the injury. A radiograph with AP, lateral and mortise views are typically sufficient in detecting a foot or talocrural joint fracture. [3] A CT Scan tin can be used to get a three dimensional view in the case of a suspected fracture. A bone scan can be used to detect small-scale fracture or stress fractures within the beginning 24-48 hours, which may not exist picked upward by a radiograph or CT scan. [1] Common fracture areas for the human foot and ankle are at the malleoli, 5th metatarsal and calcaneus. Malleolar fractures are typically dependent upon the human foot position and management of force. Metatarsal fractures typically occur with trauma, rotational forces or repetitive stress. Fractures of the calcaneus can occur with falls. [three]
Reading a radiograph for a fracture of the malleolus [edit | edit source]
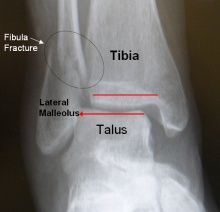
Lateral malleolus fracture AP view
Reprinted from http://www.footeducation.com/ankle-fracture-surgery
- Discover lack of congruency in a bone and/or a low radiodensity black line through the bone.
Reading a radiograph for a 5th metatarsal fracture [edit | edit source]

X ray of fifth metatarsal (Jones) fracture
Reprinted from http://en.wikipedia.org/wiki/Jones_fracture
- Observe lack of congruency in a bone and/or a low radiodensity black line through the bone.
Reading a radiograph for a calcaneus fracture [edit | edit source]

Lateral view radiograph of a calcaneal fracture
Reprinted from http://en.wikipedia.org/wiki/File:Calcaneus_Fracture.jpg
- Using a lateral view in non-weight bearing observe lack of congruency in a os and/or a low radiodensity blackness line through the os.
Reading a bone scan for a stress fracture [1] [edit | edit source]

Bone scan for 2nd metatarsal stress fracture
Reprinted from http://www.aafp.org/afp/2003/1015/p1527.html
- Find increased uptake of the radioactive compound at the expanse of injury.
- In acute injuries the uptake may be more focal, while in chronic injuries the uptake could exist throughout the os
Posterior Tibial Tendinopathy [edit | edit source]
When a clinical exam indicates suspected posterior tibial tendinopathy that may require surgical intervention an MRI is considered the "gold standard" for imaging. MRI imaging for posterior tibial tendinopathy tin can be taken with T1 and T2 weighted images. Contrast can besides be used to raise the image. The foot is typically held in a neutral position and sagittal and axial images are taken of the tendon. Colour sonography can likewise been used to detect posterior tibial tendinopathy. Imaging is performed with the patient in prone. The tendon is imaged from posterior to the medial malleolus to the tendon insertion at the navicular. AP and transverse diameters are achieved by modifying the position of the transducer head. While MRI is considered the "gold standard", ane study showed that when comparing ultrasound to MRI, ultrasound had high specificity and sensitivity in diagnosing tendinopathy and peritendinosis.[vi]
Reading MRI for Posterior Tibial Tendinopathy [6] [edit | edit source]

Axial view of T1 weighted MRI enhanced with contrast
Reprinted from http://www.ajronline.org/content/178/i/223/F9.expansion.html
- Detect an increment in signal intensity on T1 and T2 weighted images in the involved area
- Increased AP diameter of the tendon that creates a rounder tendon
- Increased indicate intensity around the peritendinous tissue indicated peritendinosis
Reading a sonograph for posterior tibial tendinopathy [half dozen] [edit | edit source]
![]()
Transverse view of sonogram of the posterior tibial tendon
Reprinted from http://www.ajronline.org/content/178/one/223/F12.expansion.html
- Discover mixed echogenic fibers and increased flow in the involved tendon
- Increased AP diameter creating a rounder tendon
- Peritendinosis can be indicated by hyperechoic tissue effectually the tendon or increased menses in the peritendon
References: [edit | edit source]
- ↑ i.0 ane.one one.2 ane.3 Swain J, Bush-league Thou. Diagnostic Imaging for Concrete Therapists. St. Louis: Saunders Elsevier; 2009; pg 152, 187
- ↑ 2.0 2.1 Lee KM, Ahn Southward, Chung CY, Sung KH, Park MS. Reliability and Relationship of Radiographic Measurements in Hallux Valgus. Clinical Orthopedics and Related Research; 2012
- ↑ 3.0 3.1 three.2 3.3 3.4 Houck J, Neville C, Chimenti R. The Foot and Ankle: Physical Therapy Patient Direction Utilizing Current Show. Current Concepts of Orthopedic Physical Therapy 2012; iii: 30-31
- ↑ 4.0 4.1 4.two Oae K, Takao U Y, Ochi G. Evaluation of Anterior Talofibular Ligament injury with stress radiography, ultrasonography and MR imaging. Skeletal Radiol. Aug fifteen 2009; 39 (i): 41-47
- ↑ 5.0 5.1 5.2 Sheyerer M, Helfet D, Wirth South, Werner C. Diagnostics in suspicion of Talocrural joint Syndesmotic Injury. Am J Orthop. 2011; xl(4): 192-197
- ↑ 6.0 half-dozen.1 six.2 Premkumar A, Perry MB, Dwyer AJ, Gerber LH, Johnson D, Venzon D, et al. Sonography and magnetic resonance imaging of posterior tibial tendinopathy. Am J Roentgenol, 2002; 178: 223-32
Source: https://www.physio-pedia.com/Diagnostic_Imaging_of_the_Foot_and_Ankle_for_Physical_Therapists
0 Response to "How to Read a Mri of Ankle Posterior"
Post a Comment